Beware deteriorating consciousness after any head injury that initially produced no LOC or after initial drowsiness seems to have resolved. This lucid interval pattern is typical of extradural bleeds
Causes/Factors
Any tear in dural venous sinus will result in extradural bleed
- Suspect after any traumatic skull fracture - often fractured temporal or parietal Bone causing lacerating to middle meningeal artery (pterion)
Symptoms
- Loss of Consciousness: Often followed by a period of lucidity (a brief return to consciousness) before deteriorating.
- Severe Headache: Often localized at the site of impact.
- Nausea and Vomiting: Resulting from increased intracranial pressure.
- Confusion: Altered mental state and disorientation.
- Weakness or Paralysis: Typically on one side of the body.
- Unequal Pupils: Anisocoria, due to pressure on the brain.
Signs
- Lucid Interval: A period of consciousness between the head injury and the onset of symptoms. This may last hours to days before a bleed declares itself by falling GCS
Diagnostic Tests
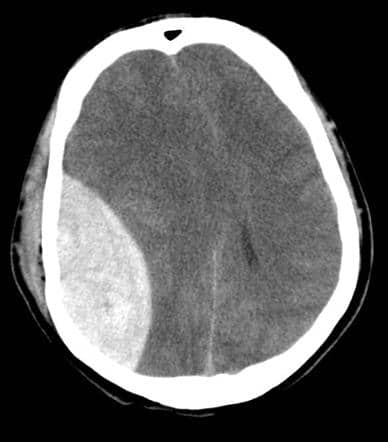
- CT Scan: Imaging to visualize the hematoma and assess its size and location.
- Skull XR may be normal or show fracture lines
LUMBAR PUNCTURE IS CONTRAINDICATED due to ICP
Management
Extradural Hematomas are considered surgical emergencies, and treatment involves:
- Craniotomy: Surgical removal of the hematoma to relieve pressure on the brain.
- Medications: To control symptoms, manage seizures, and reduce brain swelling.
Complications/red Flags
Poor prognosis if not diagnosed and operated on quickly
- Increased Intracranial Pressure: Can lead to brain herniation, a life-threatening condition.
- Neurological Deficits: Depending on the size and location of the hematoma.