1. Patient details
- Name, DoB
- When the CXR was taken
- Where it was taken
- Any previous images for that patient
2. Quality of image - PE
Projection - is it supine or erect? (almost all will be AP). Erect in cases of suspected perforation
Exposure - needs to be adequate to assess small and large bowel
3. Bowel and other organs
Differentiating small bowel vs large
- Small bowel lies more centrally - large bowel extends to the periphery
- Small bowel’s mucosal folds are visible across the full width of the bowel. The large bowel “folds” (haustra) only extend partially across the width. There may be causes however when it does extend across the whole length of the bowel.
- Faeces have a mottled appearance and are most often visible in the colon due to trapped gas within it.
3/6/9 rule The upper limits for the different bowel segments: Small bowel: 3cm Colon: 6cm Caecum: 9cm
Other organs and structures
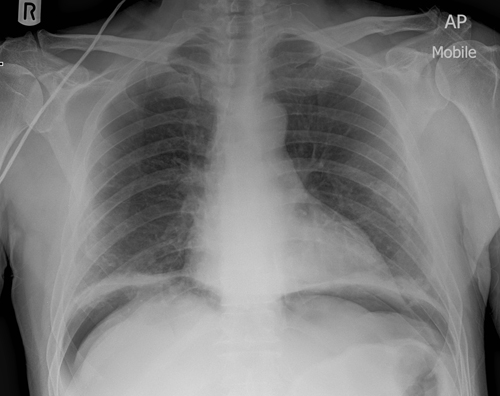
- Lungs: inspect the lung bases for pathology (e.g. consolidation) as abdominal pain can, in some cases, be caused by basal pneumonia.
- Liver: a large right upper quadrant structure.
- Gallbladder: rarely visible on an abdominal X-ray, however, you should quickly inspect for calcified gallstones and cholecystectomy clips.
- Stomach: visible between the left upper quadrant and midline, containing a variable amount of air.
- Psoas muscles: the lateral edge is marked by a relatively straight line either side of the lumbar vertebrae and sacrum.
- Kidneys: both are often visible, the right kidney is lower than the left due to the presence of the liver on the right.
- Spleen: located in the left upper quadrant, superior to the left kidney.
- Bladder: has a variable appearance depending on the fullness of the bladder.
4. Bones
Take a quick look at the bones for pathology:
- Ribs
- Lumbar vertebrae
- Sacrum
- Coccyx
- Pelvis
- Proximal femurs
5. Calcification and artefact
Various high density (white) areas of calcification or artefact may be noted on abdominal X-ray including:
- Calcified gallstones in the right upper quadrant
- Renal stones/staghorn calculi
- Pancreatic calcification
- Vascular calcification
- Costochondral calcification
- Contrast (e.g. following a barium meal)
- Surgical clips
Presentations
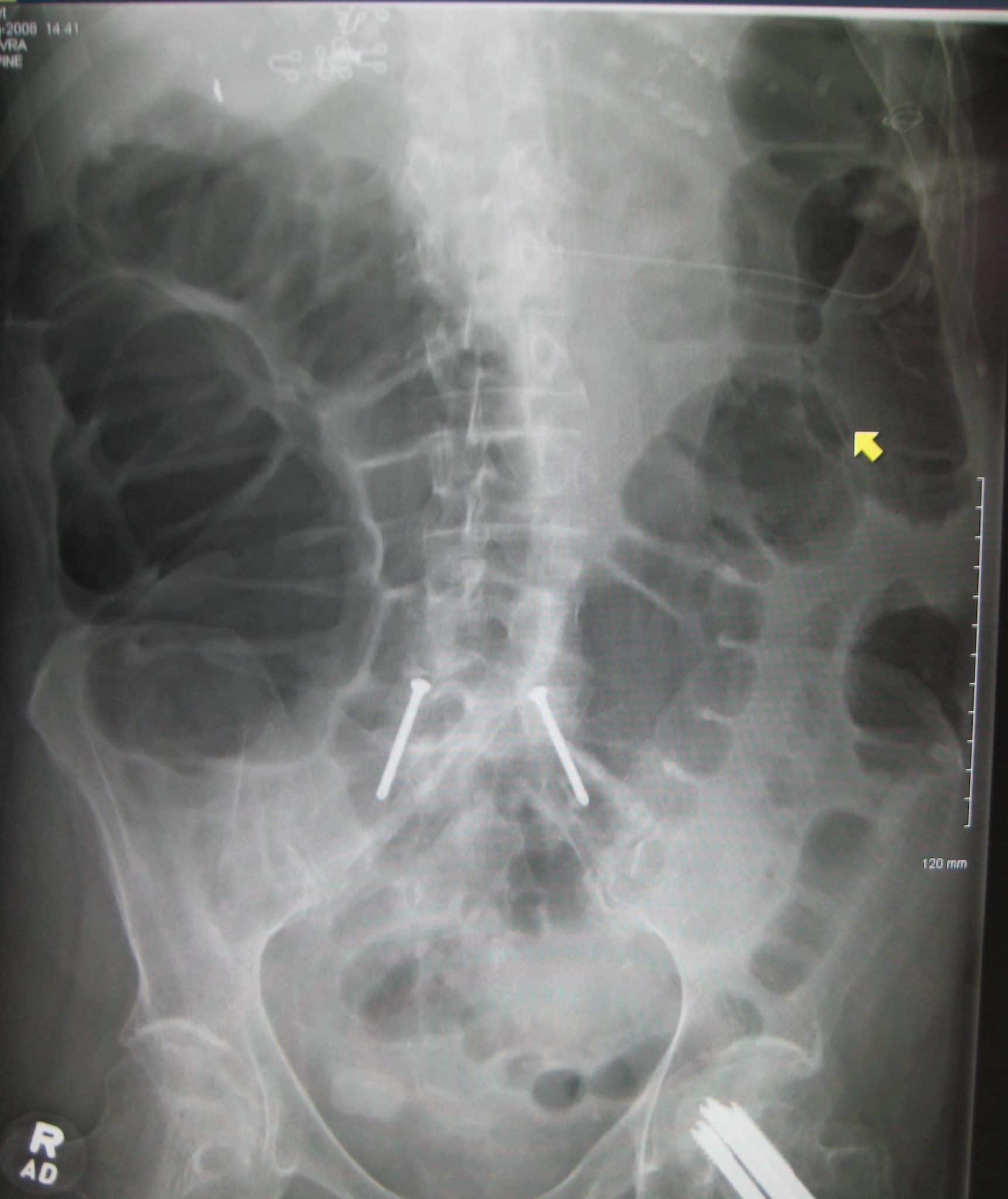
Small bowel obstruction
- Dilation of the small bowel
- Prominent valvulae connivents creating a coiled spring appearance
- Adhesions are the most common cause of small bowel obstruction - 75%. Abdominal hernias (10%)

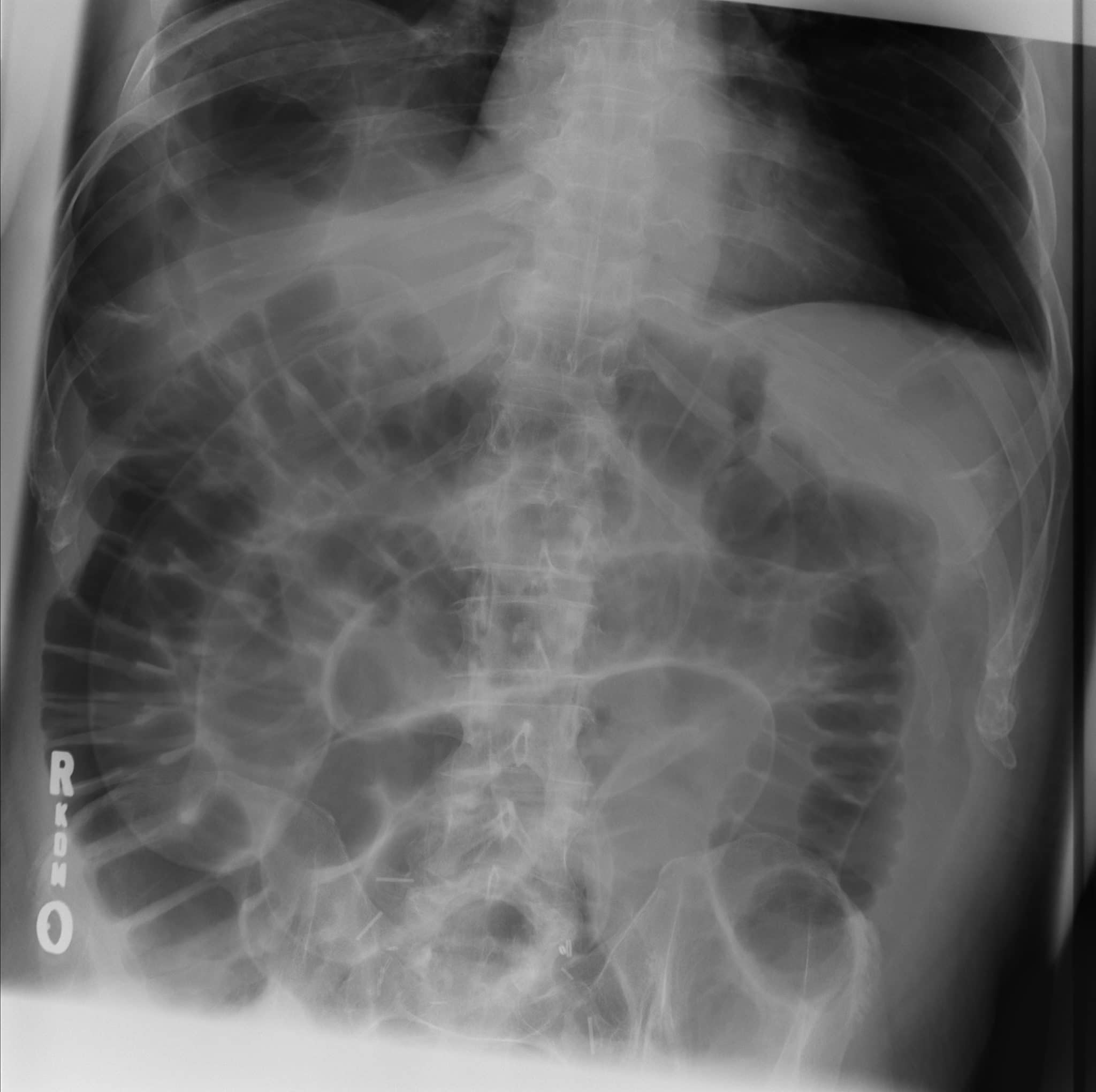
Large bowel obstruction
Most common cause is colorectal carcinoma and diverticular strictures. Less commonly hernias and volvulus.
Large bowel obstruction
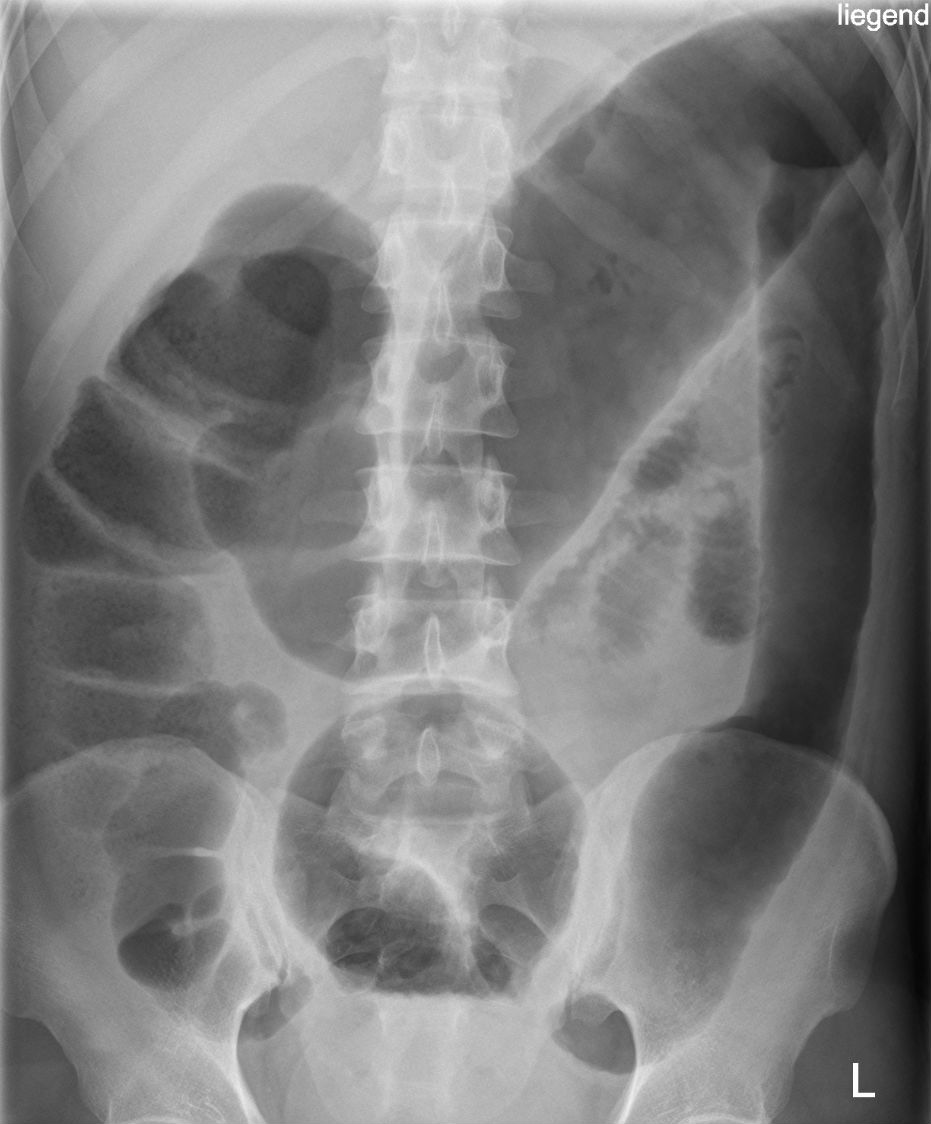
Volvulus is a twisting of the bowel on its mesentery and most commonly occurs at the sigmoid colon or caecum. High risk of bowel perforation and/or bowel ischaemia.
- Sigmoid volvulus - coffee bean appearance
- Caecal volvulus - often described as having a fetal appearance
 |  |
|---|---|
| Sigmoid volvulus | Caecal volvulus |
Rigler’s (double wall) sign
The inner wall of the bowel should only be visible on an abdominal XR. The presence of free air within the abdomen (pneumoperitoneum) can result in both sides of the bowel wall becoming visible.
Causes of pneumoperitoneum - perforated bowel, perforated duodenal ulcer, recent abdo surgery.
Pnmeumoperitoneum
Rigler’s sign
Inflammatory bowel disease
Features on XR include:
- Thumbprinting: mucosal thickening of the haustra due to inflammation and oedema causing them to appear like thumbprints projecting into the lumen.
- Lead-pipe (featureless) colon: loss of normal haustral markings secondary to chronic colitis.
- Toxic megacolon: colonic dilatation without obstruction associated with colitis.
Toxic megacolon in a patient with Ulcerative Colitis. Note the lead-pipe colon with loss of the normal haustral folds due to chronic colitis