Urinary tract calculi/stones
Stones forming in the lumen of the urinary tract, anywhere from renal calyx bladder. Types:
- Calcium 70% - raised calcium
- Urate 5% - raised urate, gout etc
- Cystine 1% - raised cystine eg congenital cystinuria
- Struvite 15% - raised pH of urine so magnesium ammonium phosphate salts precipitate out
Causes/Factors
-
Raised associated mineral
- Hypercalcaemia eg parathyroid adenoma
- Raised urate eg gout
-
Dehydration
-
Stagnant urine
Leads to soluble material to precipitate out
Clinical Features
Pain - excruciating
-
URETER: Classic “loin to groin” pain - renal colic
-
BLADDER: lower abdo pain
-
URETHRA: dysuria
-
Haematuria
-
Reduced UO
Diagnostic Tests
- Urine dip - haematria + look for infection
- U&Es - kidney function, calcium levels
- USS/CT - negative ultrasound does not exclude diagnosis
Management
Symptoms
Opiates not effective
- NSAIDs - Diclofenac - IM or rectal
- IV Paracetamol if NSAIDs contraindicated
- Anti-emetics - Metoclopramide, prochlorperazine, cyclizine
- Antibiotics if infected
Stone
Watch and wait approach if less than 5mm in diameter as there is a 50-80% chance of these passing on their own. May also be appropriate to wait for 5-10mm depending on other factors.
- -blocker tamsulosin can facilitate spontaneous stone passage during the waiting period. Only for stones less than 10mm
- Surgical intervention for large stones or stones that do not pass on their own. Also indicated in cases of complete obstruction and infection
- Shockwave lithotripsy (SWL) - break up stone to pass
- Ureteroscopy + laser lithotripsy
- Percutaneous nephrolithotomy - under GA
To prevent recurrence
-
2.5-3L of water a day
-
Lemon juice in water - citric acid binds to urinary calcium
-
Avoid carbonated drinks - phosphoric acid promotes calcium oxalate formation
-
Reduce salt intake
-
Maintain normal calcium intake - too low intake can also increase risk
-
Potassium citrate + Thiazide diuretics for patients with recurrent calcium stones
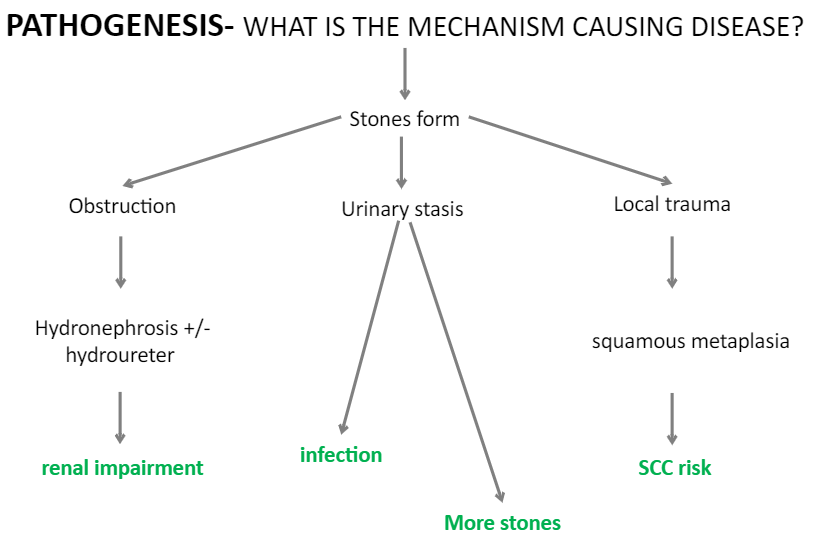
Complications/red Flags
- Infections