When the lack of Insulin or Insulin sensitivity causes a starvation state in the body despite excessive glucose. - the ketoacidosis pathway.
The combination of both acidosis and hyperglycaemia can be deadly
Typically in Type 1 DM very rarely in type 2
Causes/Factors
- Insulin Deficiency: Often due to missed Insulin doses or inadequate Insulin therapy.
- Infection or Illness: Infections or other illnesses can increase the body’s need for Insulin.
- Undiagnosed Diabetes: In some cases, DKA may be the first sign of diabetes.
- Stress or Trauma: Physical or emotional stress can contribute e.g.
- Infection
- Surgery
- MI
- pancreatitis
- Certain Medications: Such as corticosteroids, wrong Insulin dose, antipsychotics
Symptoms
- Gradual drowsiness
- Polyuria
- Polydipsia
- Nausea and Vomiting
- Abdominal Pain:
- Fruity Breath Odor: Due to the presence of ketones.
- Confusion or Altered Mental Status
Diagnostic Tests
- Acidaemia (venous pH <7.3 or HCO3 < 15mmol/L)
- Hyperglycaemia (> 11mmol/L or known to have Diabetes Mellitus)
- Ketonaemia (> 3mmol/L or ++ on dipstick)
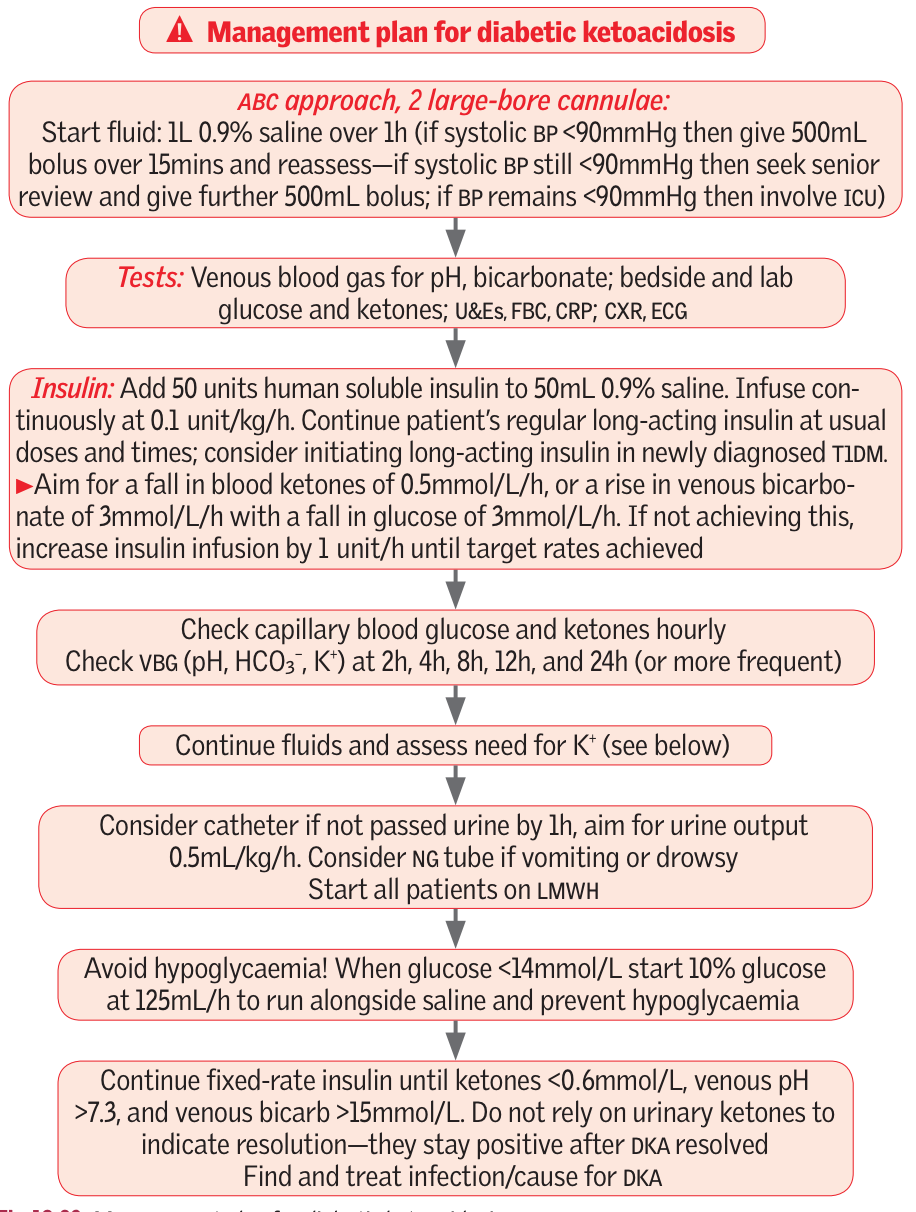
Management
Complications/red Flags
Red flags - get senior help!
If one or more of the following features is present on admission consider transfer to ICU/HDU for monitoring and central venous access
- Blood ketones > 6mmol/L
- Venous HCO3 < 5mmol/L
- Potassium < 3.5mmol/L
- GCS <12
- SpO2 <92% on air (assuming no respiratory disease)
- Systolic <90
- Pulse >100 or <60
- Anion gap above 16
Complications
-
Cerebral oedema - watch for fall in GCS
-
Aspiration pneumonia
-
Hypo -kalacemia, -magnesaemia and -phosphataemia
-
Plasma glucose is usually high but not always especially if Insulin continued
-
High WCC may be present without an infection
-
Often no fever with an infection
-
Some creatinine assays cross-react with ketones so may not get a true renal picture
-
Serum amylase is often raise and non-specific abdo pain is common even without a pancreatitis