Reducible - the contents of the hernia can be manipulated back into their original position through the defect. Left alone or repaired electively
Incarcerated or Irreducible - the contents are stuck and cannot be pushed back into their original position. Acutely incarcerated hernias should be repaired urgently
Obstructed - the contents of the hernia containing bowel are compressed to the extent that the bowel lumen is no longer patent. Colicky, abdominal pain, distension, distension, vomiting and absolute constipation are cardinal features.
Strangulated - compression of the contents of the hernia by the fascial defect prevents blood flow into the tissues, causing ischaemia.
Causes
Increased intra-abdominal pressure, weak or damage tissues
Increased intra-abdominal pressure:
- Chronic cough - COPD, long-term smoking, bronchiectasis, Cystic Fibrosis
- Abdominal distension - Pregnancy, Ascites, peritoneal dialysis, Obesity
- Straining - chronic conception, prostatism, heavy lifting during work
- Kyphoscoliosis
Weakened tissues
- Congenital defects - patent processus vaginalis, patient umbilical ring
- Collagen disorders - EDS, vitamin C deficiency, FH
- Trauma - including surgery
- Ageing
- Chronic Malnutrition
- Long-term corticosteroid use
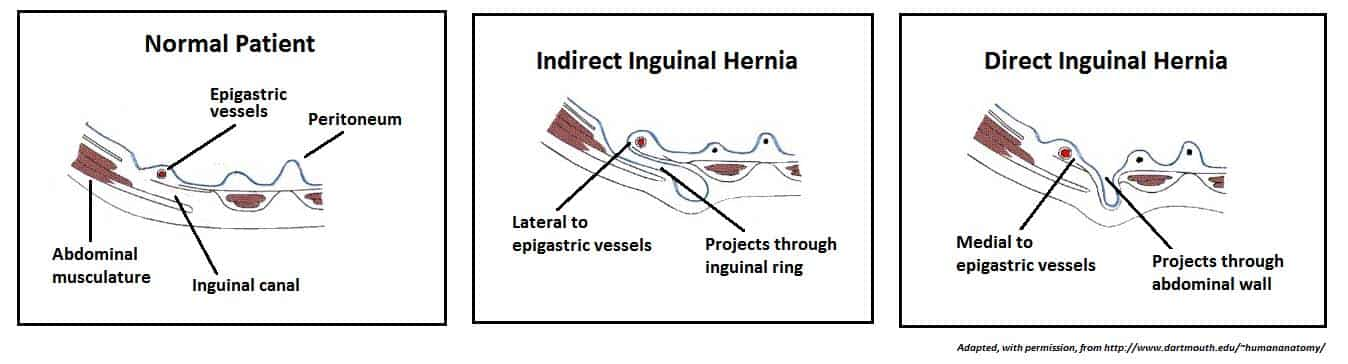
Inguinal hernia
Most common type of hernia - 70% of all hernias. Inguinal ligament runs from the ASIS to the pubic tubercle
In men, it transmits the spermatic cord to the testis, and in women, it contains the round ligament. In both sexes, it also carries the ilioinguinal nerve and the genital branch of the genitofemoral nerve.
Direct - weakness in posterior wall of inguinal canal - medial to deep ring. Contents are forced directly through this defect into the inguinal canal.
Indirect - enter the deep ring, pass along the length of the inguinal canal
Both types exit via the superficial ring. It is much more common for indirect hernias to form a inguinoscrotal hernia (as less resistance)
To tell the difference between the two, if you press the deep ring and the hernia still protrudes the hernia is a direct hernia
- Much more common in older men
- Low BMI - Obesity seems to be protective
- Superior and medial to pubic tubercle (to differentiate from femoral)
Can be managed via open or laparoscopic surgery with a mesh.
Hiatal hernias
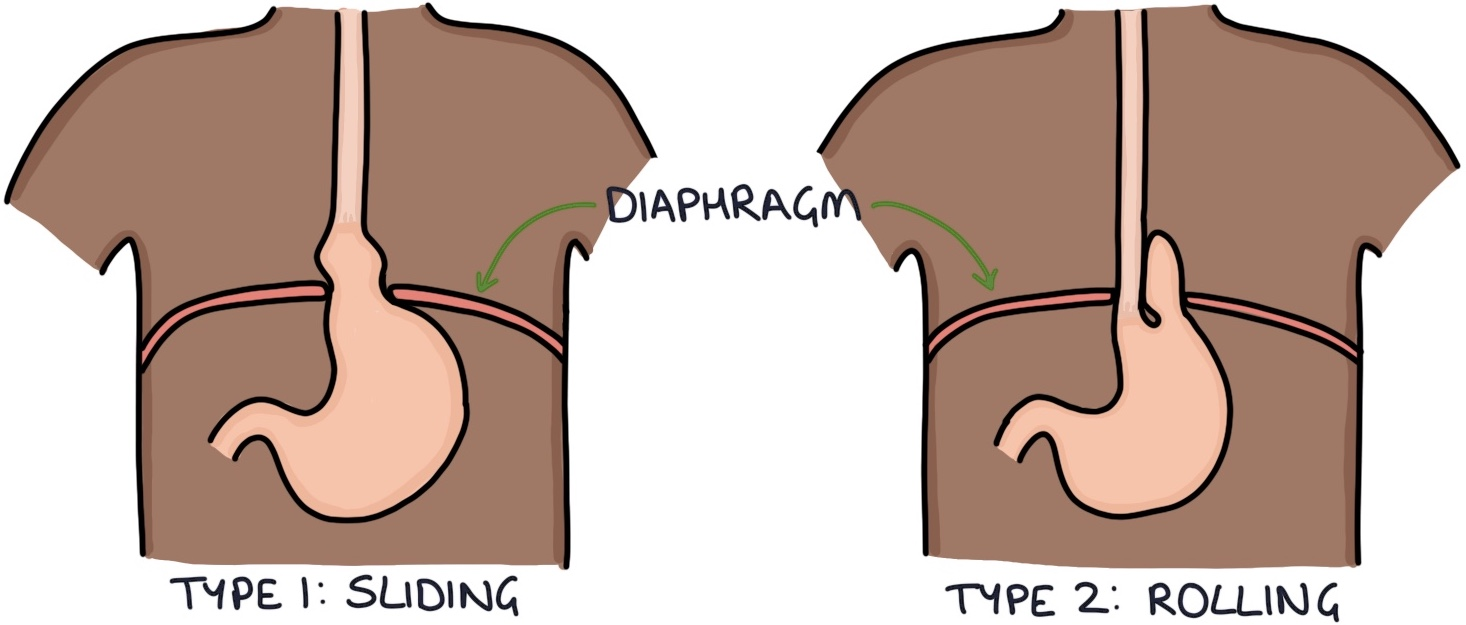
Herniation of the stomach/abdominal contents through the oesophageal hiatus of the diaphragm.
The sliding type is very common and usually only involved the top part of the stomach sliding upwards. This impairs the function of the lower oesophageal sphincter leading to Gastro-oesophageal reflux disease and related symptoms.
- Often found incidentally on endoscopy or CXR
Para-oesophageal type can involved stomach and other abdominal organs herniating around the oesophagus. This may result in life-threatening complications and can be difficult to repair

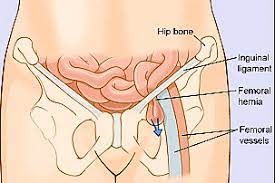
Femoral hernia
Less common than groin hernia but frequently present with Bowel Obstruction.
- More common in older women
- low BMI
- previous laparoscopic inguinal hernia repair is a protective factor
- Can become incarcerated much more easily than inguinal
- Lateral and inferior to pubic tubercle
Due to the high risk of complications femoral hernias should always be repaired - laparoscopic mesh
Umbilical hernia
Most common ventral hernia. Protrusion through a fascial defect in or around the umbilical ring.
True (direct) hernia - congenital problem when the ring fails to close
Paraumbilical (indirect) hernia - associated with acquired fascial defect in the linea alba within 3cm of the umbilical ring
- Most common in women especially during or after Pregnancy
- More likely to cause problems that require surgery in men
- Down’s syndrome and Beckwith-Widemann syndrome increased incidence
- Increased abdo pressure - Obesity or Ascites
Usually asymptomatic - usually report long standing lump. Can usually be managed conservatively.
Obturator hernia
Very rare and difficult to diagnose clinically.
- “Little old lady hernia”.
- Especially common in people who are very thin or recently lost weight
More than 90% present as an emergency with an Acute Abdomen and features of Bowel Obstruction. The deep position of the hernia means there is hardly ever a lump.
Needs emergency surgery