Factors that disrupt the mucus barrier or increase stomach acid increase the risk of ulceration
Causes/Factors
Mucus barrier disruption
- Helicobacter pylori
- NSAIDs
Increase stomach acid
- Stress
- Alcohol
- Caffeine
- Smoking
- Spicy foods
Bleeding risk from ulcer
- NSAIDs
- Aspirin
- Anticoagulants
- Steroids
- SSRIs
Presentation
- Epigastric discomfort
- Nausea and vomiting
- Dyspepsia
- Haematemesis
- Coffee ground vomit
- Melaena
- Iron deficiency Anaemia
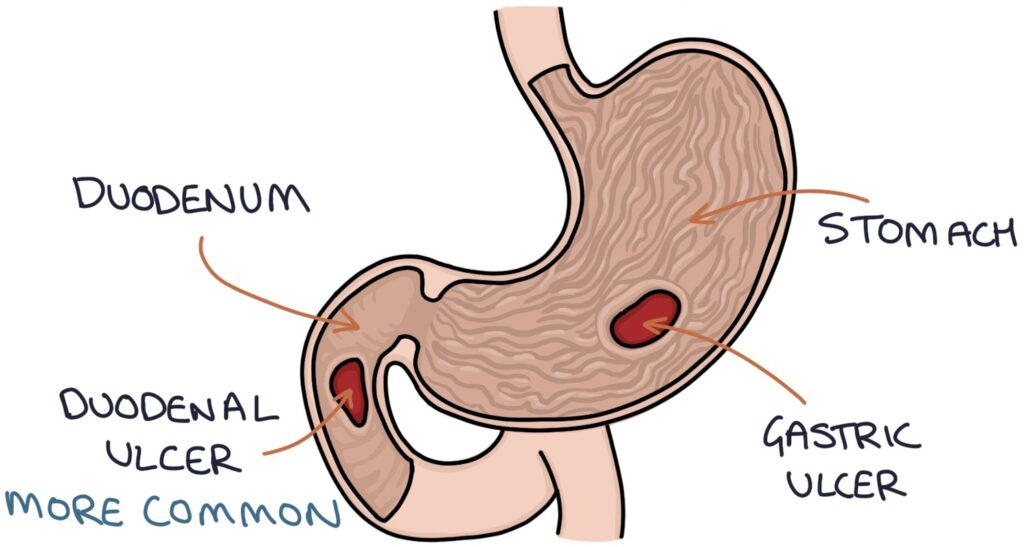
Gastric vs duodenal ulcers differentiating history
- Eating typically worsens the pain of gastric ulcers - so patients tend to lose weight due to the fear of pain on eating
- Duodenal ulcer pain tends to improve after eating so weight stays the same or increases
Investigations
- OGD - endoscopy. During endoscopy a rapid urease test can be used to check for H. pylori infection. A biopsy can also be considered to exclude malignancy.
- Stool sample - H pylori PCR
- PR exam - to check for melena
Management
- Stopping NSAIDs
- Treating H pylori infection - TDS Amoxicillin 1g and clarithromycin 500mg or Metronidazole 400mg
- Proton pump inhibitor to reduce gastric acid secretion - lansoprazole 30mg, Omeprazole 20-40mg, etc
Complications/red Flags
- Significant bleeding
- Perforation - acute abdo pain and peritonitis requiring urgent surgery
- Scarring and strictures - pyloric stenosis (early fullness after eating and upper abdo discomfort)