Note for this page
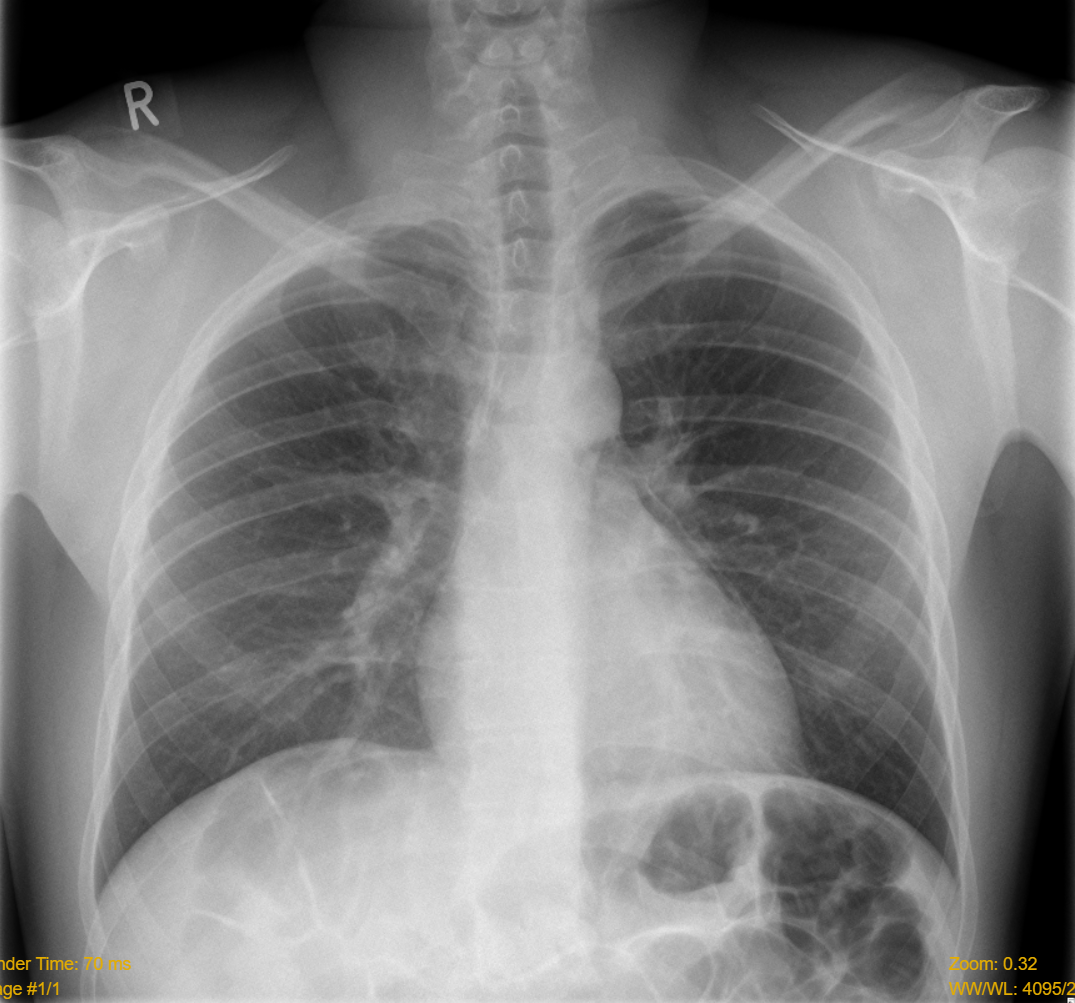
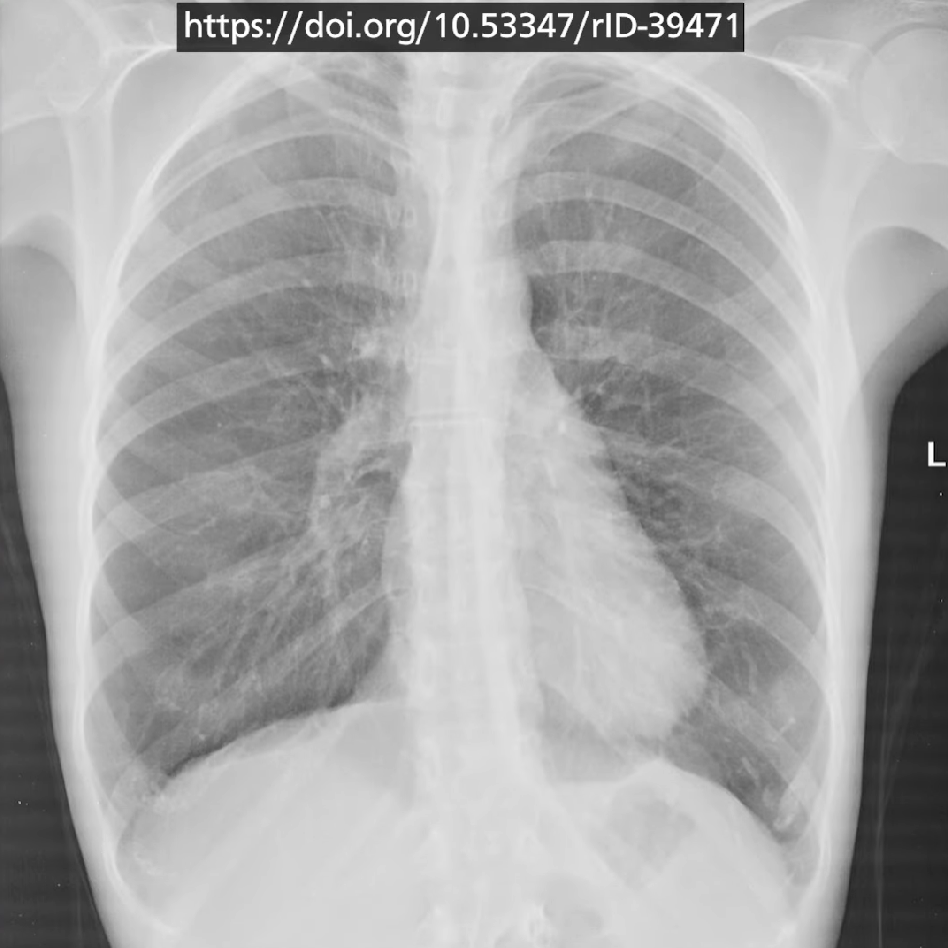
All of the images will have no pathology unless indicated otherwise
Quick check
1. Patient details
- Name, DoB
- When the CXR was taken
- Where it was taken
- Any previous images for that patient
2. Quality of image - RIPE
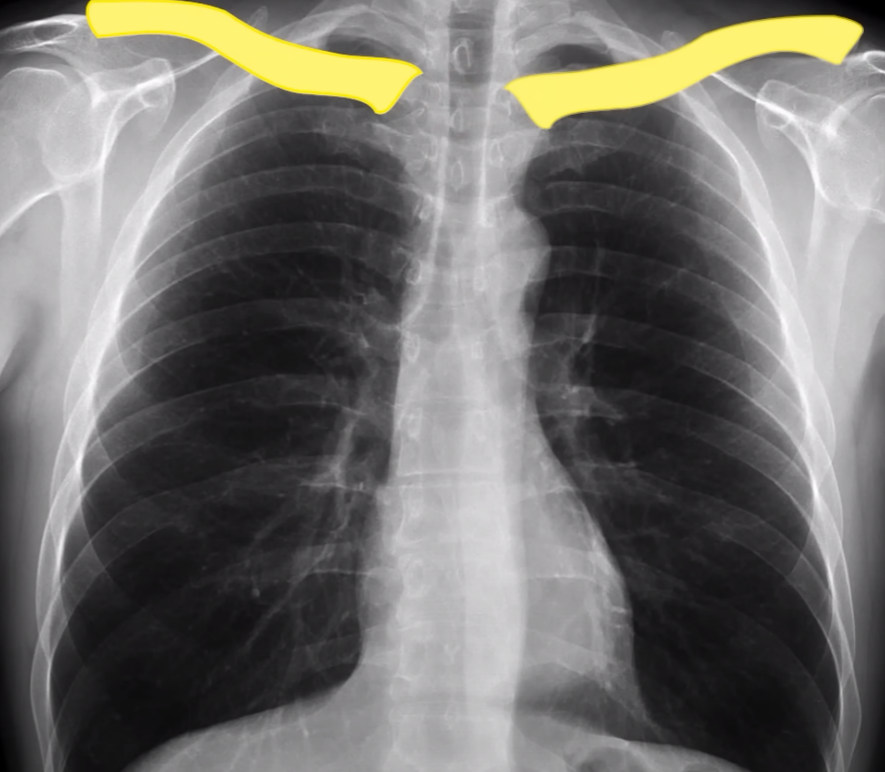
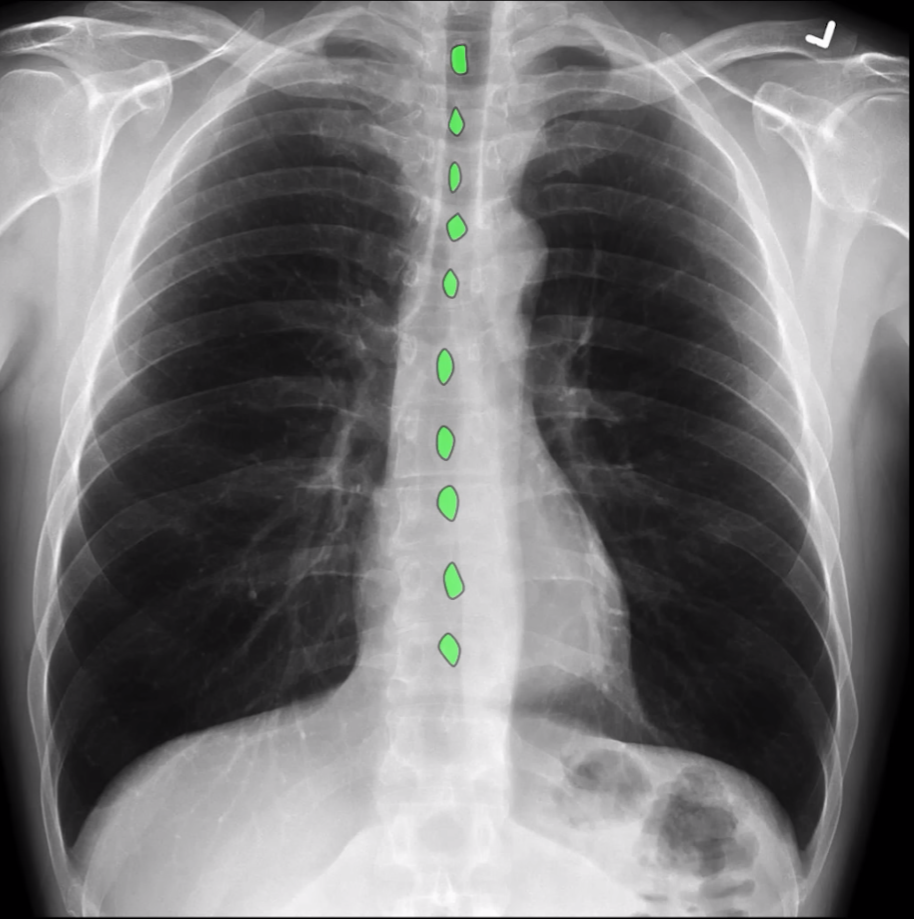
Rotation
- The medial parts of the two clavicles should be equal distance from the spine
- Spinous processes should be vertical
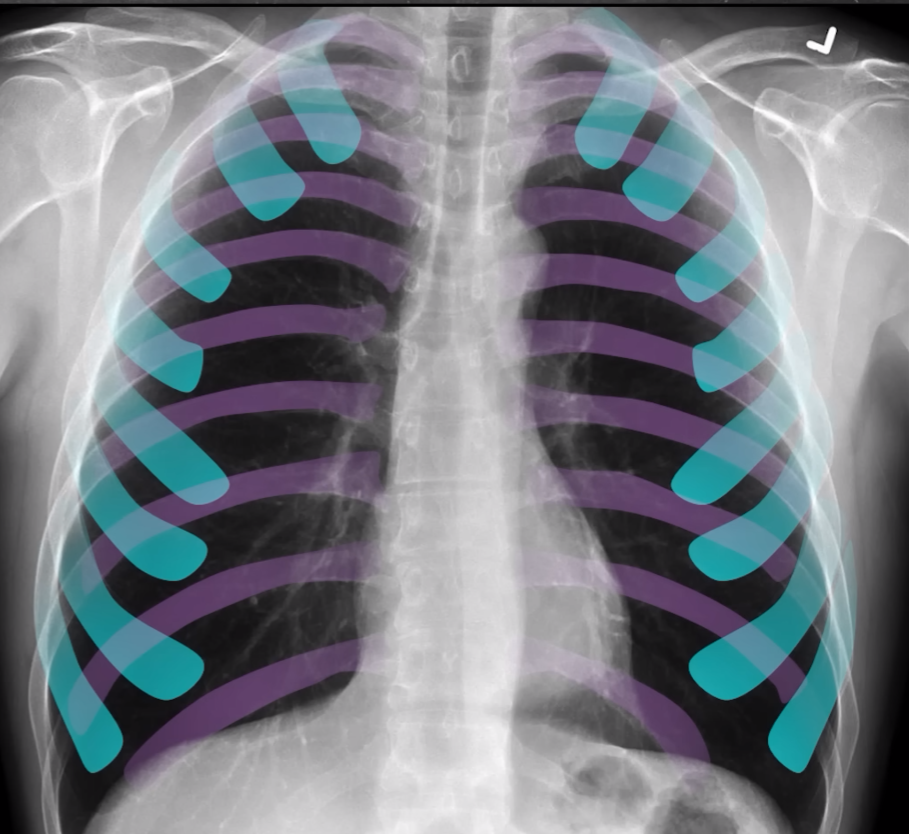
Inspiration
- 5 to 7 anterior ribs or at least 9 posterior ribs
- Inspiratory effort could be gauged
- Poor inspiration can mimic cardiomegaly
- Crowding of vessels at the base of the lungs can mimic consolidation or collapse and often occurs in acutely unwell patients
Projection
- AP/PA?
- Most CXR are PA as AP misrepresent the size of the heart (too large)
- Can tell if AP if scapulae projected over lung fields
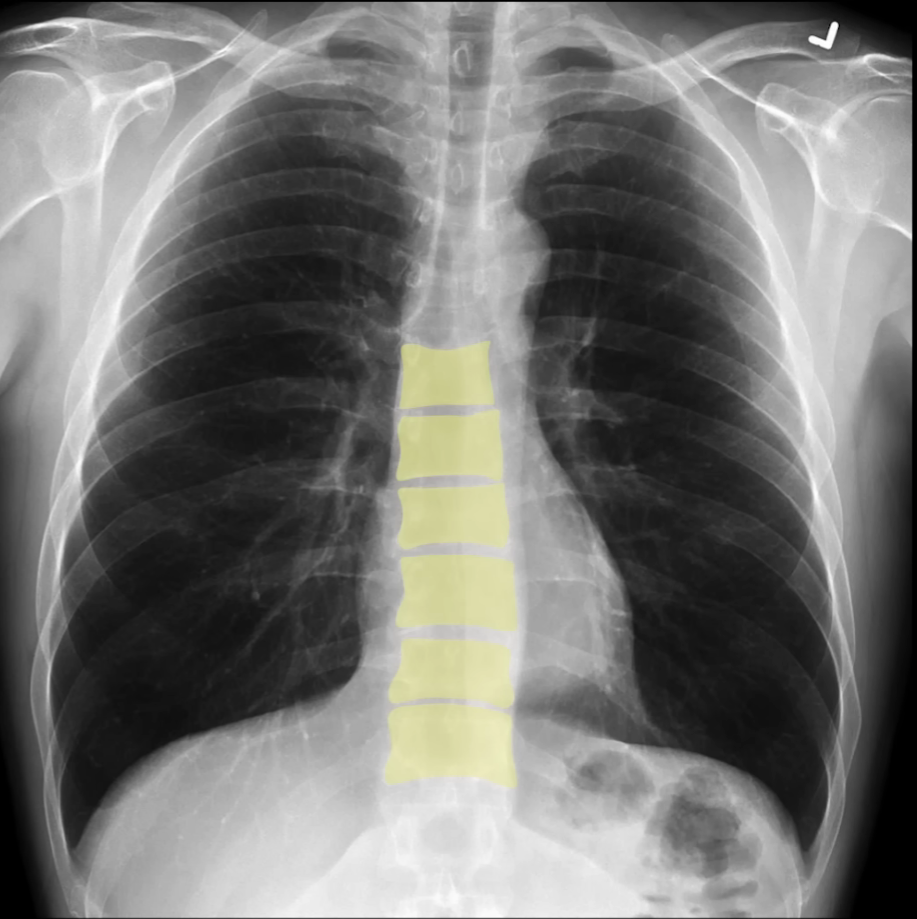
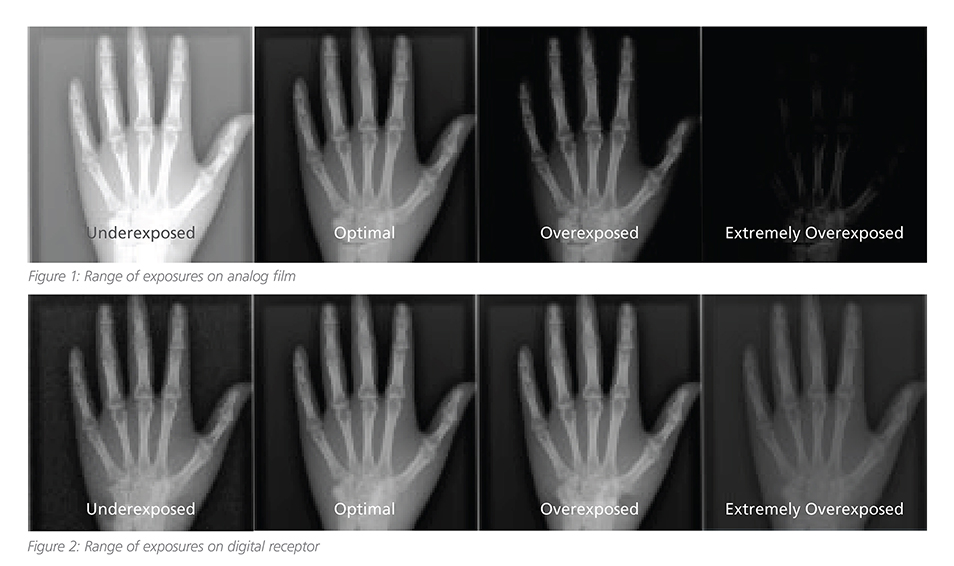
Exposure
- Correct definition and quality in image.
- Can tell if can see vertebrae behind the heart
3. Clinical findings - ABCDE
Airway
- Trachea
- PUSH - any increase in volume - significant pneumothorax or Pleural Effusion exhibit mass effect
- PULL - loss in volume - lung collapse
- Carina and bronchi
- Right bronchus is straighter and wider than the left risk for aspiration
- Hilar regions
- Check for abnormal vessels, or enlarged lymph nodes
- Right hilar should always be higher than left
- Bilaterally enlargement suggests Tuberculosis or Sarcoidosis
- If unilateral think Lung Tumours
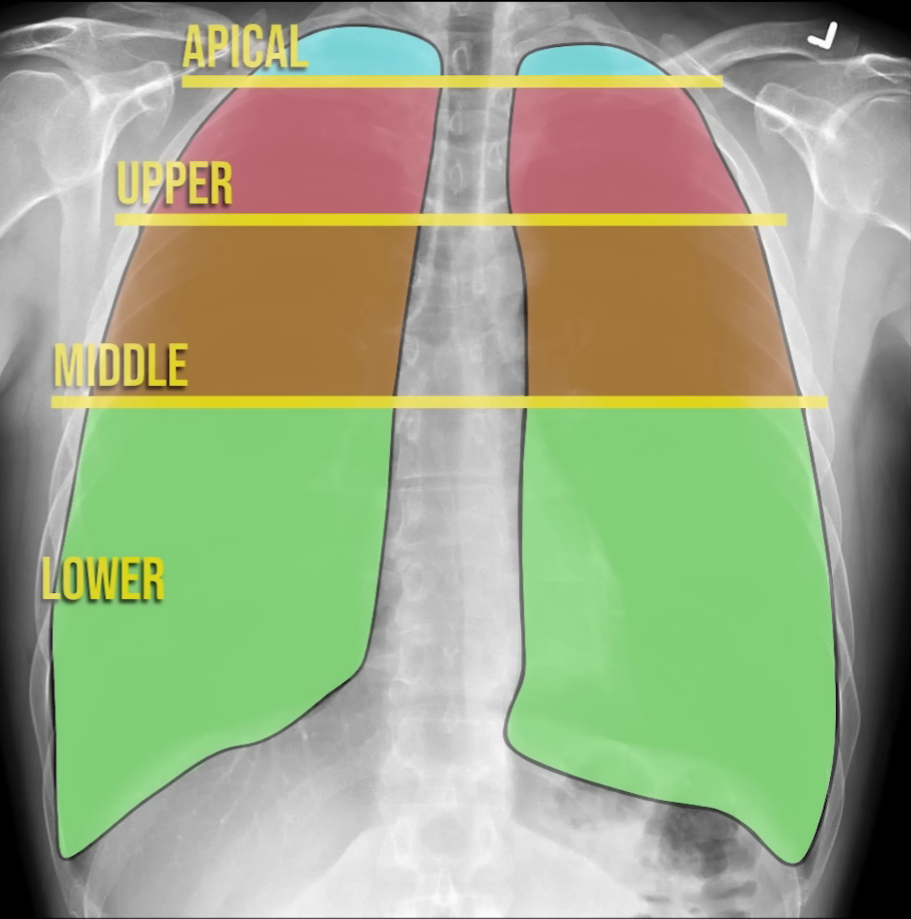
Breathing
Zones are used instead of lobes when localising a lesion
Lack of any lung markings pneumothorax
Pleura are only visible if they become thickened or fluid accumulates (e.g. mesothelioma)
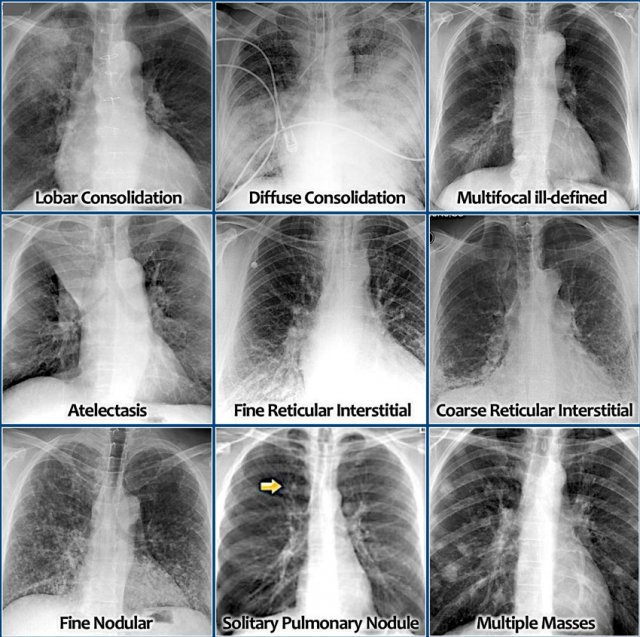
Lung opacities are described as nodular, reticular (network of fine lines, interstitial) or alveolar (fluffy). A single nodule may be called a space-occupying lesion
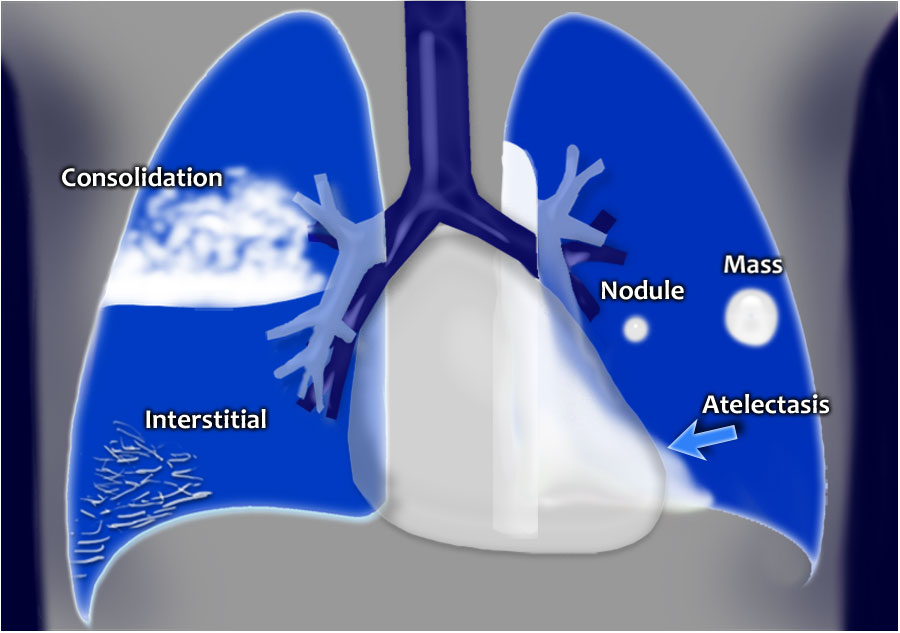
Nodules - if >3cm across it becomes a pulmonary mass
- Neoplasia: metastases, lung cancer, hamartoma, adenoma
- Infections: varicella pneumonias, septic emboli, abscess, hydatid
- Granulomas: Tuberculosis, Sarcoidosis, histoplasmosis
- Pneumoconiosis (except asbestosis)
Reticular opacification - lung parenchymal changes
- Acute interstitial oedema
- Infection: acute (viral, bacterial), chronic (TB, histoplasmosis)
- Fibrosis: interstitial pneumonia, drugs (methotrexate, Bleomycin, crack cocaine), connective tissue disorders, systemic sclerosis, Industrial dust diseases, interstitial lung disease

Alveolar opacification - can be due to any material filling the alveoli
- Pus - pneumonia
- Blood - haemorrhage, DIC
- Water - heart, renal or Liver failure, ARDS, smoke inhalation, heroin, toxicity, near drowning
- Cells - Lymphoma, adenocarcinoma
- Protein - alveolar proteinosis, ARDS, fat emboli

Ring opacities - either from a CT cross section referring to bronchiectasis/bronchitis or cavitating lesions on CXR
Linear opacities - septal lines (Kerley B lines, i.e. interlobular lymphatics seen with something), atelectasis, pleural plaques
White out of whole hemithorax - pneumonia, large Pleural Effusion, ARDS, post pneumonectomy
Cardiac
- Should be less than 50% of the overall thoracic window
- Boarders should be clearly defined - usually consolidation would change this
- Consolidation of the lingula blurs the left heart boarder
- 1/3 should lie to the right of the vertebral column, 2/3 to the left
- May appear elongated if the chest is hyperinflated COPD or enlarged in AP or if there is LV failure or pericardial effusion
Diaphragm
- The right side is often slightly higher due to liver
- Costophrenic angles should be well defined and acute
- Blunting can be caused by hyperinflation of fluid collections
Everything
- Damage to bony structures
- Dislocations
- Lytic lesions
- Presence of extra features - double left heart boarder (left lower lobe collapse)
- Breast shadows or lack of them
- Artificial shadows: wires/leads/tubes/artificial valves/pacemakers/past sternotomy
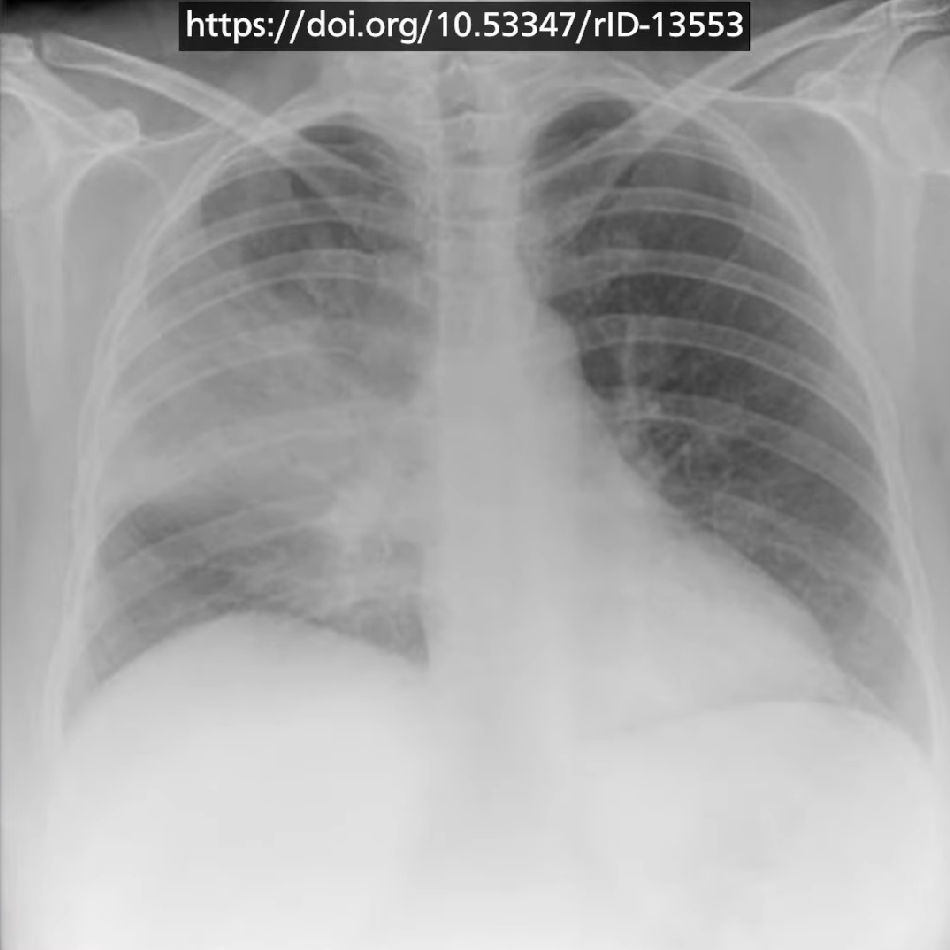
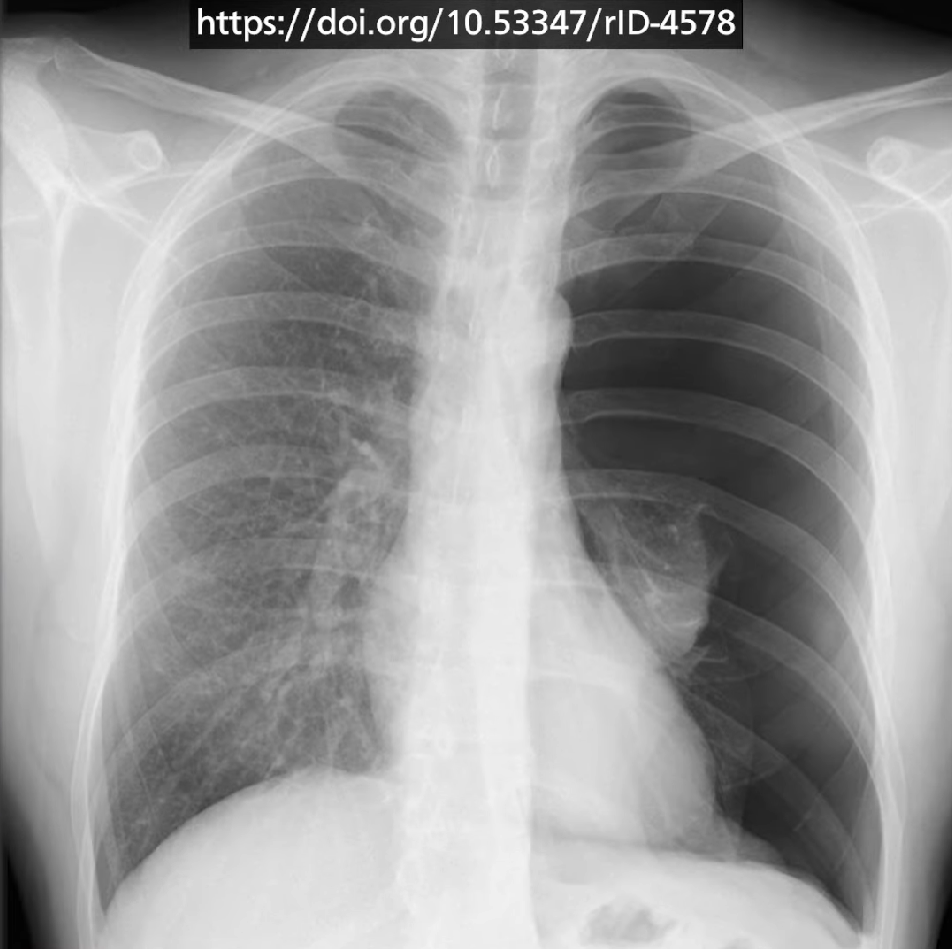
Examples of pathological scans
Lobar pneumonia (typical Strep. pneumoniae)
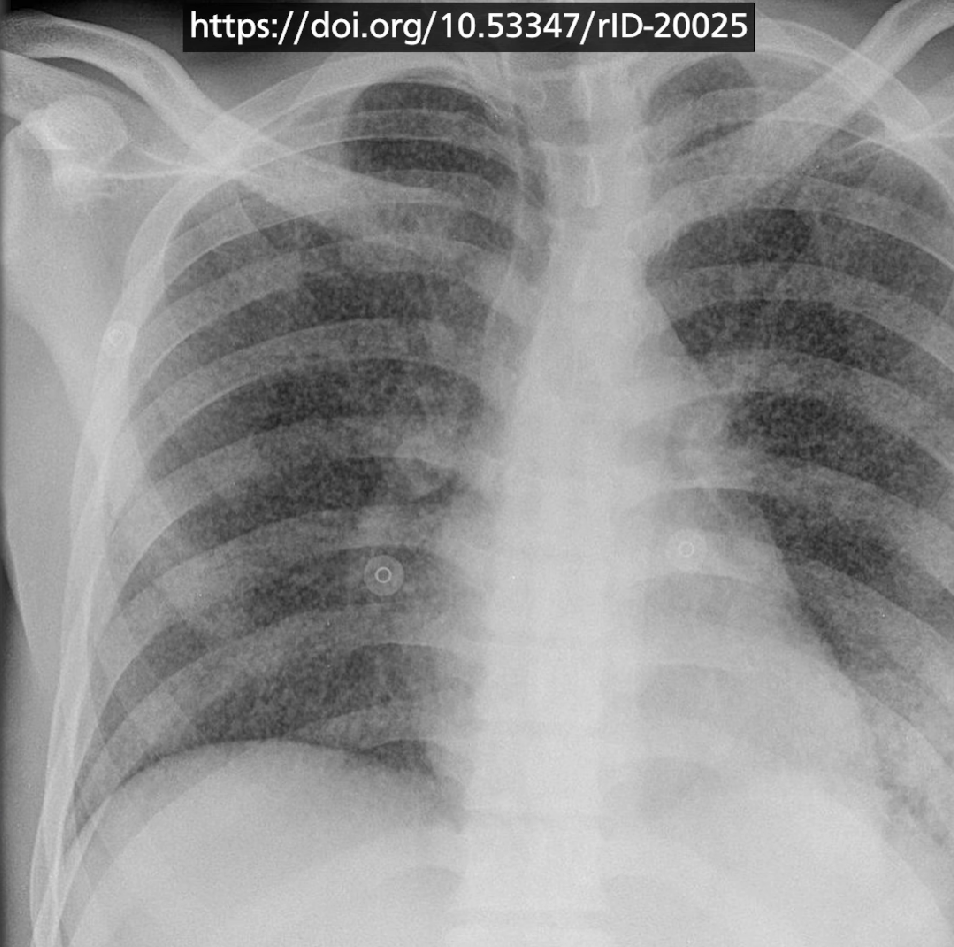
Atypical pneumonia (mycoplasma)
Aspiration pneumonia (can move depending on position)

Tuberculosis
Ghon lesion - left middle lobe Calcified lymph nodes

Miliary tuberculosis
Uncontrolled haematogenous spread
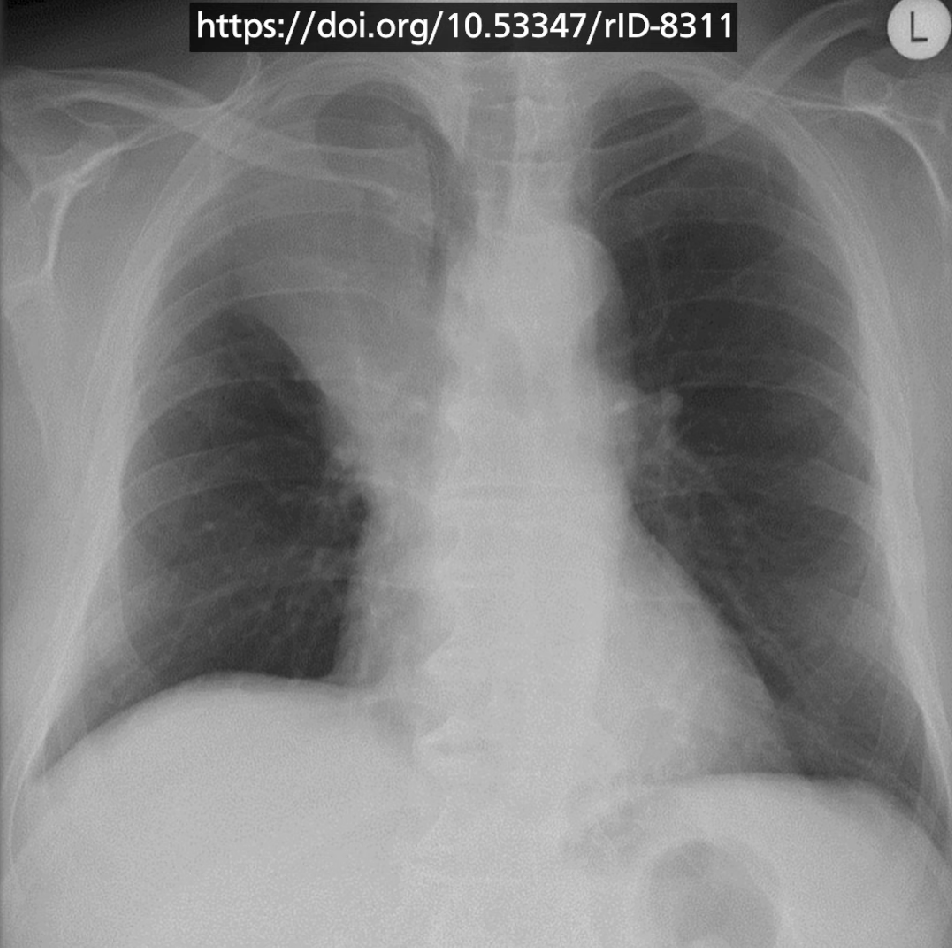
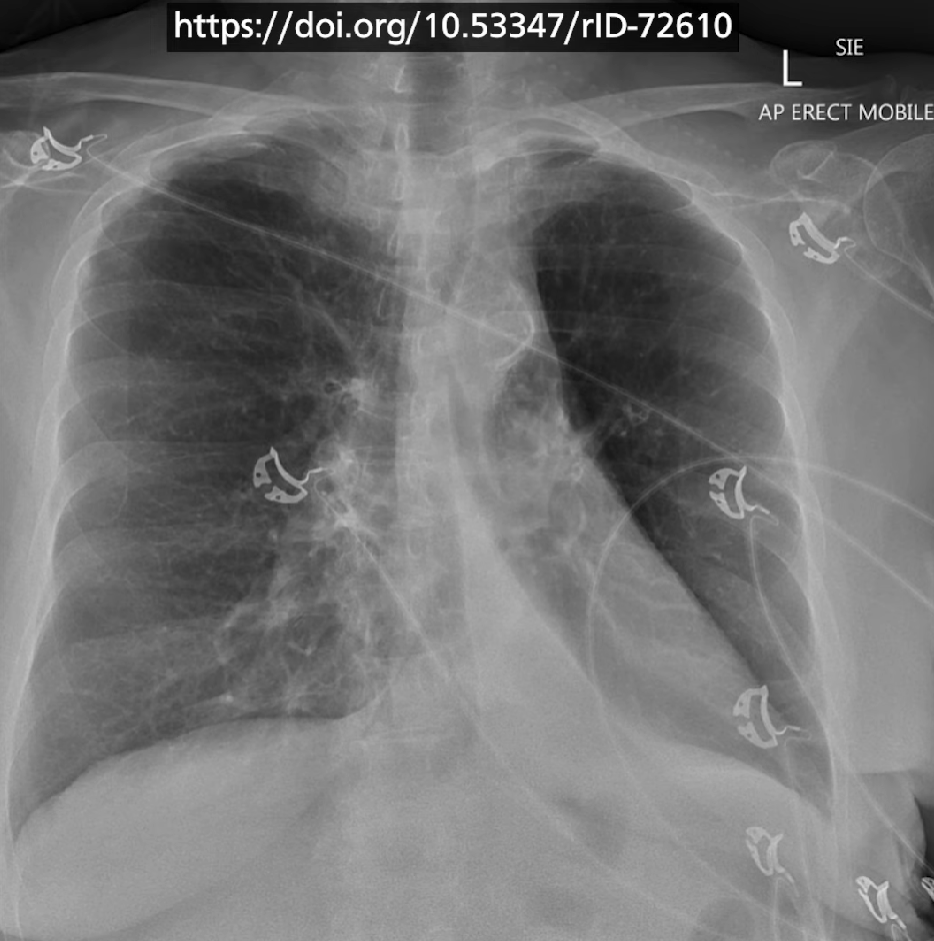
pneumothorax
Hydropneumothorax
Pneumomediastinum
Lobar collapse
Right middle zone collapse - loss of RHB and in lateral view
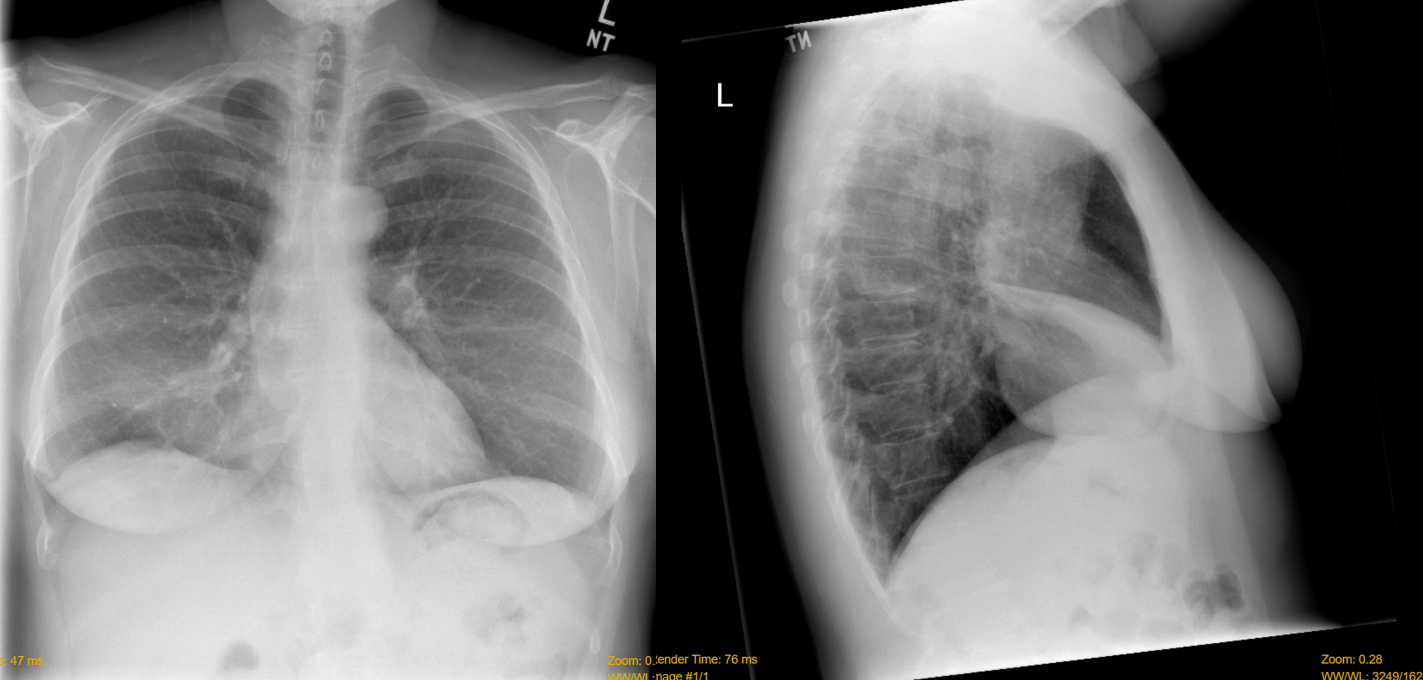
Sail sign - left lower lobe collapse
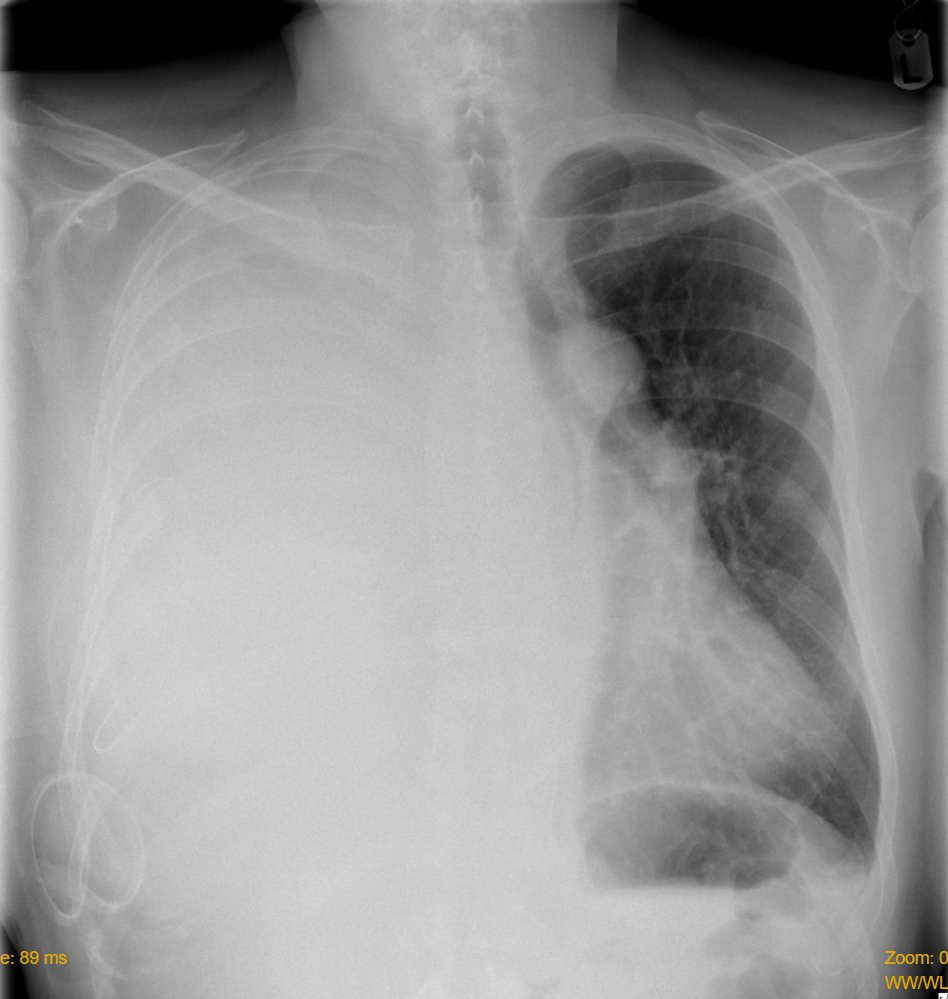
Pleural Effusion
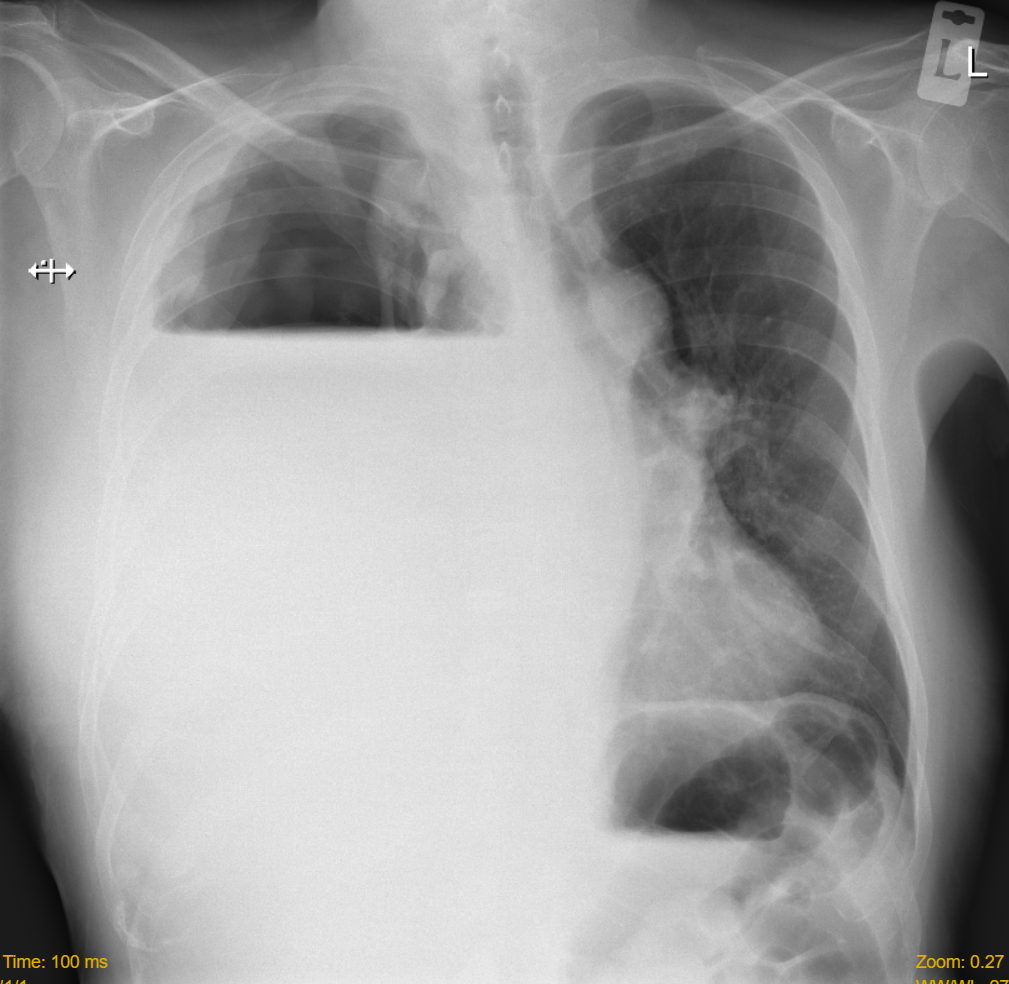
pneumonectomy (no mass effect - volume loss)
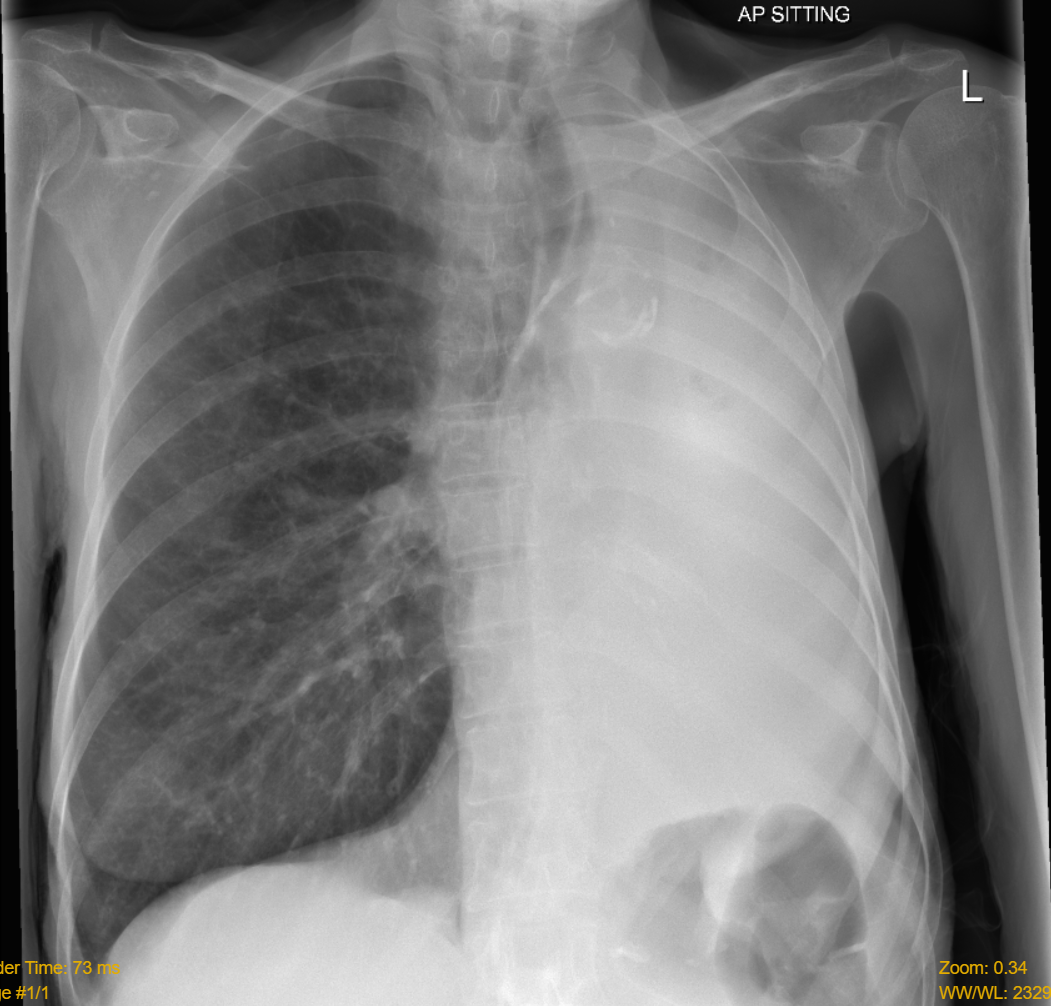
Massive Pleural Effusion (with mass effect)
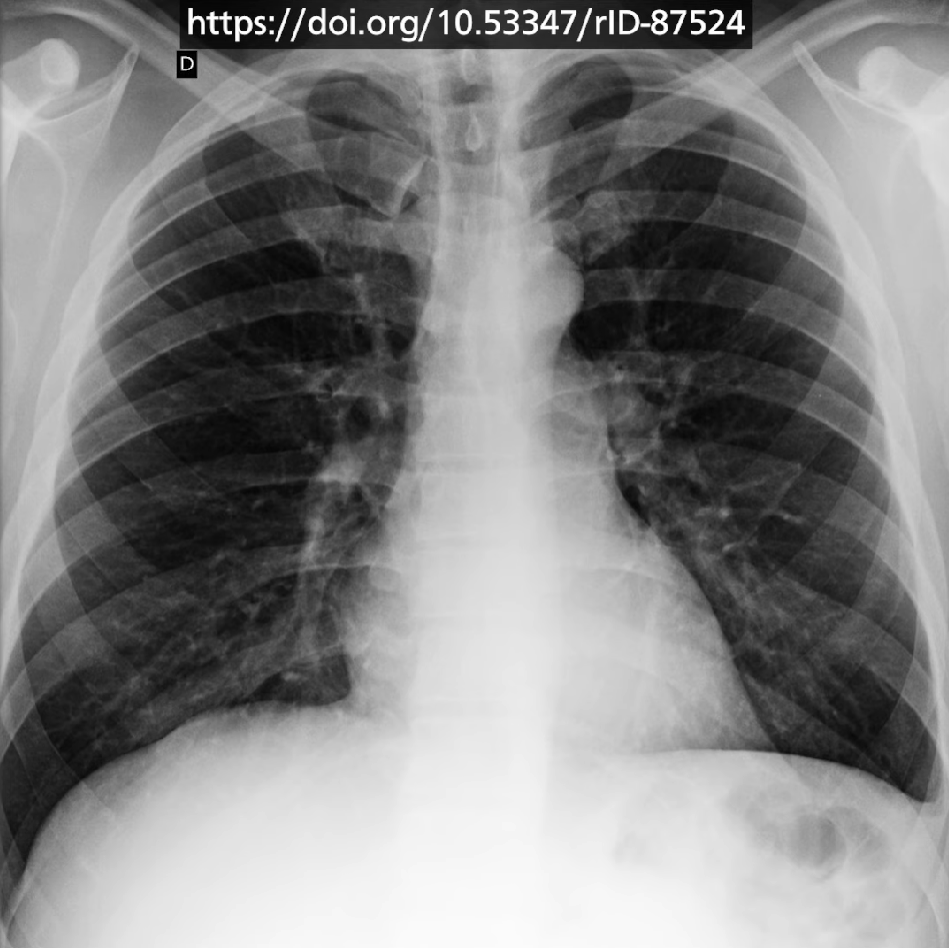
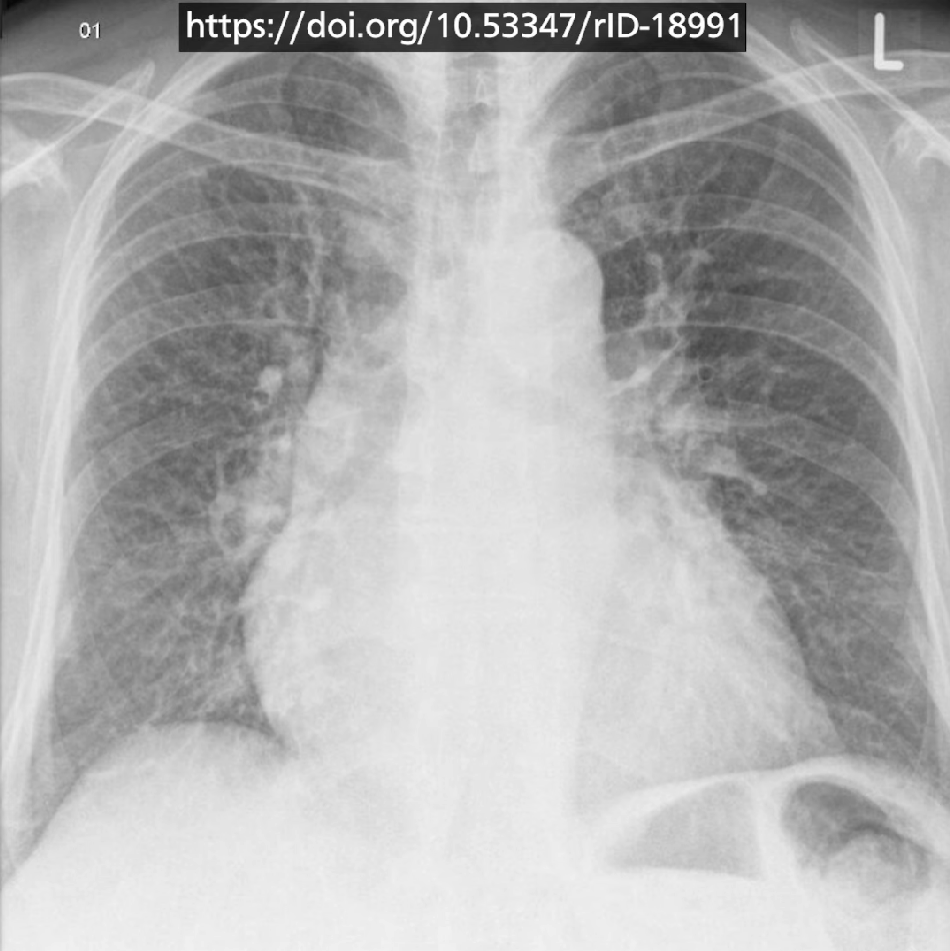
COPD
- Flattened diaphragm
- More anterior ribs seen
- May see floating heart sign
- Bullous emphysema
Heart Failure
- Alveolar oedema - bat wing opacities in middle
- (Kerley) B lines - thickened interlobular septum which extend inwards. Horizontal line that extends to the periphery
- Cardiomegaly
- Dilated upper lobe vessels
- Pleural Effusion
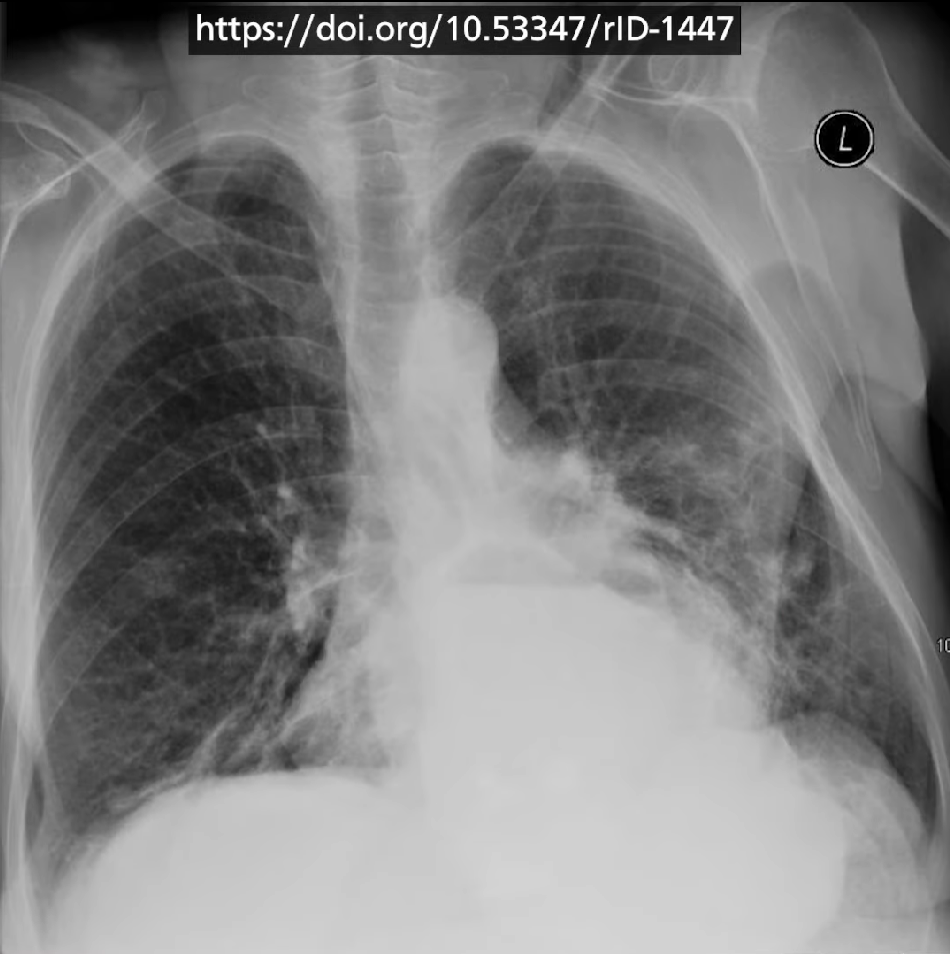
Hiatus hernia
Lung Tumours
Cannonball mets - from primary breast cancer Pancoast tumour Horner’s Syndrome
Check ribs for invasive lesion